
By STEVEN MERAHN, MD

In 1807, in an effort to spite the British and French for shipping interference (and forced recruitment of American citizens into military service), the United States Congress passed an Embargo Act, effectively shutting down trade with these two countries. Britain and France quickly found other trading partners; the US, then limited in our capacity to sell products outside our borders, was left with a devastated economy and a gaping hole in our face. It took only weeks before Congress passed a loophole; they repealed the act within 15 months of its passing. It was a great lesson in unintended consequences.
Today, ignoring history, both Republicans and Democrats seem to spar continuously around healthcare: whether the message is about tearing down the Affordable Care Act or about some version of Medicare (For-All, For Whoever Wants It, For America, or For Better or Worse), both parties are terribly wrong.
Assuming the social imperative for healthcare is to eliminate preventable morbidity and disability (and associated costs) and improve (or sustain) quality of health of all our citizens (in order to help as many of them as possible remain productive, contributing members of society), another approach to ‘universal care” would be to flip the figure/ground relationship for our current efforts: instead of developing better payment systems, let’s develop and commit to a universal clinical operating framework that ensures that every member of society has the same opportunity to optimize their health status.
“Centralizing” the methodology around a universal model for how we plan for care, and allocate resources to ensure care plan goal achievement, would be far more valuable to society than centralizing the sources of funds to pay for care, because then we’d know what we’re paying for.

While Federal mandates may smell to some like limits on personal liberty, more than 70% of American healthcare expenses are already not paid by patients themselves; 20% are subsidized by employers and 50% (or more in the case of citizens over age 65, families with children at risk and adults with special needs) are paid out of Federal and State government coffers. This means we are paying for each other’s care right now, and will continue to do so in one way or another.
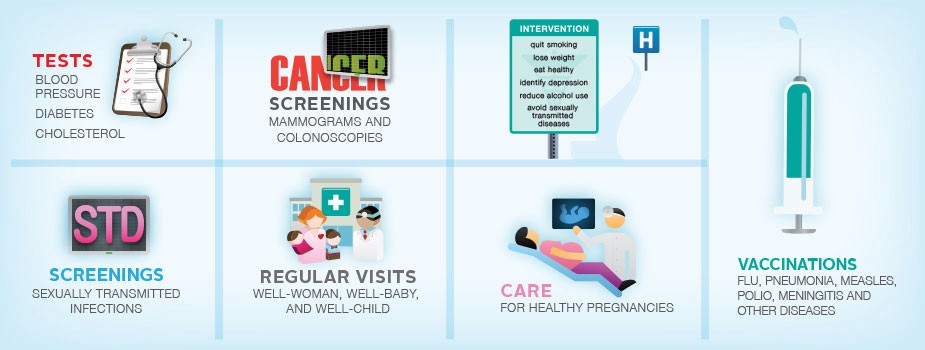
When the ACA was passed, one of the elements of that seemed most offensive to critics was its most prominent feature: Essential Health Benefits. Yet, it is the “essential health benefits” feature that holds the greatest promise to help manage health spending. Here are a few of the common critical questions that were asked:
Why should I pay for maternity and newborn care if we’re done having children?
First, your insurance premiums don’t really pay for your expenses; they are put into a pool that is used for all its “members”. Some pay more than they use, some pay less; others contribute so that there is a chunk of money available to them in case of disaster.
So, here’s the thing: sick newborns, whether the result of nature or nurture, require extensive, expensive resources, special supports and services in school and can have lifelong disabilities. However, many of these problems are easily preventable through good prenatal and newborn care. While the disabled baby may not be yours, it could be your neighbors, or drain resources from your town fire department or your grandchild’s school system budget.
So, while you may see a small reduction in your insurance premium by being able to “opt-out’ of maternity and newborn care, you are going to pay anyway, and pay far more than the additional cost of that premium.
Why should I pay for preventive and wellness services I don’t want?
Whether through Federal or state tax dollars, or contributions to non-profit hospitals, we all pay for late stage cancers, heart attacks and strokes, depression, anemia and vaccine-preventable infections such as the flu or pneumonia. “Essential health benefits” reduce many of those late-stage and catastrophic costs, freeing up money for law enforcement, community services and better roads.
Eliminating essential health benefits may result in a short-term premium savings, but the economic consequences are substantial, especially as our society ages; the ACA resulted in an increase of 8,400 diagnoses of early-stage colorectal cancer among US seniors in the period 2011–13, saving hundreds of millions of your tax dollars which would have been required for late stage treatment.
Since we’re already paying a share of the costs of our fellow citizen’s medical problems, I want to make sure that my money is being spent well, or at least not spent unnecessarily. I can’t support the freedom to delay the diagnosis of colon cancer, acquire bacterial pneumonia, or go blind from diabetes or glaucoma; I can think of a few other things I would like my taxes spent on other than a completely preventable stroke and the subsequent physical and neurological consequences. These conditions put limits on freedom that go well beyond anything imposed by the ACA.
Improving the health of Americans is not really about coverage, but about increasing the use of preventive, wellness and chronic disease management services that were part of the essential health benefits. This is where the real, big league, benefits lie; but first we need to make up for lost time (and care) for millions of people with under-managed chronic illness. Only then will the overall cost of maintaining our health will go down; and, even they don’t, we will all just be healthier and live longer.
Essential health benefits should not be viewed as an imposition, but a means to assure that our communities and our country has a better quality of health, which improves workforce productivity and economic vitality. Putting our lives at risk to defend our freedom is a fundamental aspect of American life, but this is not the same as letting people have the freedom to put their own lives at risk when the consequences, and their associated economic and social costs to us all, are completely preventable.
Steven Merahn, MD is a physician executive with experience in health policy, clinical operations and patient experience management. He is the Managing Director of Thinkwell Health and recently founded Union In Action, a non-profit focused on behavioral health integration.
This post originally appeared on Tincture here.
